
TL;DR:
- Autism meltdowns are involuntary neurological crises triggered by sensory or emotional overload. Caregivers must respond with phase-specific strategies focused on safety, calmness, and gradual recovery. Prevention through environment adjustments and routine preparation reduces the frequency and severity of meltdowns over time.
An autism meltdown is defined as an involuntary neurological crisis triggered by sensory or emotional overload, not a deliberate behavior or a choice. Understanding autism meltdowns is the first step every caregiver needs before any strategy can work. These episodes differ fundamentally from tantrums, and treating them the same way makes things worse. The Child Mind Institute confirms that meltdowns build from cumulative stress and sensory input over time, not from a single sudden event. Knowing that changes everything about how you respond.
What causes autism meltdowns?
Autism meltdown causes fall into four main categories: sensory overload, routine disruption, emotional overwhelm, and accumulated stress. Each category can trigger a crisis on its own, but they often combine. A child who slept poorly, wore an uncomfortable shirt, and then faced a schedule change at school has been absorbing stress all day before anything visible happens.
Sensory triggers are the most common starting point. Loud or unpredictable noise, bright or flickering lights, strong smells, and uncomfortable textures can push the nervous system past its limit. Emotional triggers include frustration from communication barriers, social misunderstandings, and anxiety about uncertain situations. Many autistic individuals have difficulty articulating their feelings, which means the stress builds silently until it erupts.
Common autism meltdown causes include:
- Sensory overload: crowded spaces, loud environments, scratchy clothing, strong food smells
- Routine disruption: unexpected schedule changes, substitute teachers, canceled plans
- Social stress: misread social cues, peer conflict, group settings without preparation
- Communication frustration: being unable to express needs or being misunderstood
- Accumulated fatigue: multiple smaller stressors stacking up across a day or week
Pro Tip: Keep a simple daily log noting sensory exposures, sleep quality, and mood. Patterns across two to three weeks often reveal triggers that are not obvious in the moment.
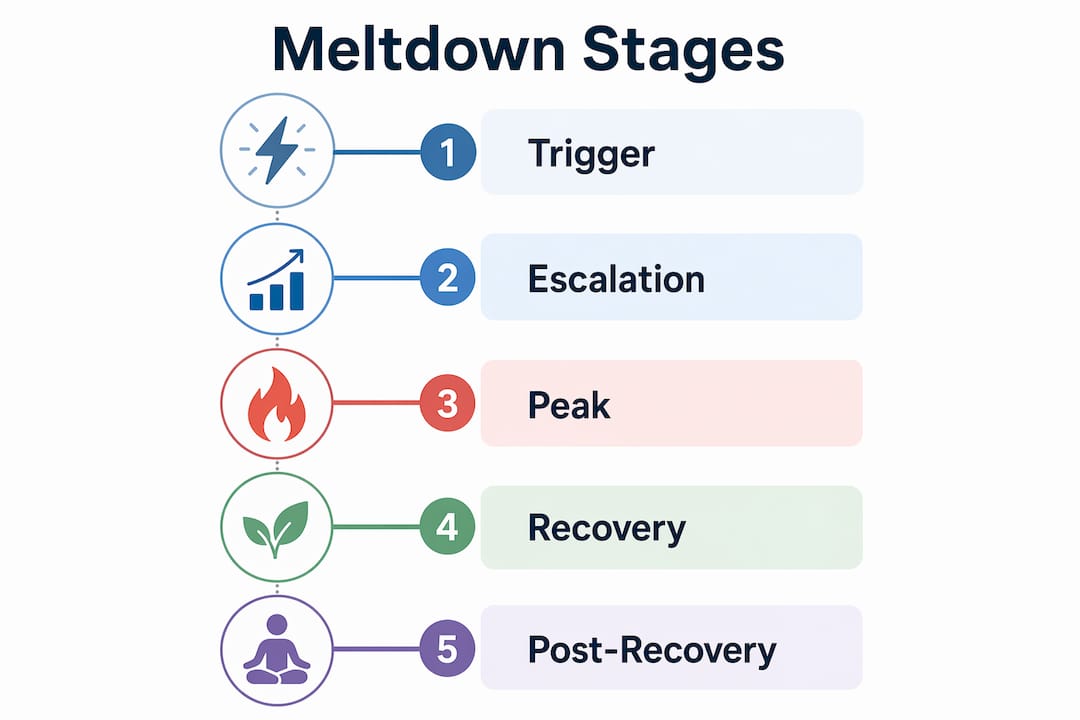
What are the stages of an autism meltdown?
Meltdowns progress through four recognizable phases. Knowing which phase you are in determines what you should do next.
- Trigger phase. A specific stressor, or the final stressor in a chain, activates the nervous system. The individual may show early signs: increased stimming (repetitive self-stimulatory movements such as rocking or hand-flapping), withdrawal, or verbal agitation.
- Escalation phase. Distress intensifies. Behaviors become louder or more physical. This is the window for early intervention. The Child Mind Institute notes that early coping skills are effective only before crisis begins.
- Crisis phase. The nervous system is in full overload. Communication is severely limited. Safety becomes the only priority. Reasoning, instructions, and questions are not processed effectively at this stage.
- Recovery phase. The nervous system gradually calms. The individual may feel exhausted, embarrassed, or emotionally raw. This phase requires patience and quiet support before any conversation begins.
| Phase | Caregiver goal | What to avoid |
|---|---|---|
| Trigger | Identify and reduce the stressor | Ignoring early warning signs |
| Escalation | Offer limited choices, reduce input | Multiple questions or commands |
| Crisis | Ensure safety, reduce sensory load | Physical contact, verbal reasoning |
| Recovery | Offer comfort, wait before talking | Immediate problem-solving or discipline |
Pro Tip: During escalation, offer no more than two options and wait a full 60 seconds between prompts. The Child Mind Institute recommends longer silences between prompts to reduce overstimulation and support the individual’s sense of control.
How are meltdowns different from tantrums and shutdowns?
Meltdowns are involuntary neurological crises. Tantrums are purposeful behaviors aimed at achieving a goal. That distinction is not semantic. It changes every response you make as a caregiver.
A child having a tantrum is aware of their audience and adjusts their behavior based on reactions. A child in a meltdown is in survival mode due to neurological overload and cannot moderate their response. Reasoning, bargaining, or consequences do not work during a meltdown because the cognitive processing required for those responses is not available. Applying discipline in this moment increases distress without changing behavior.
Shutdowns are a third, often overlooked response. Where a meltdown is an outward explosion, a shutdown is an inward collapse. The individual goes quiet, withdraws, stops responding, and may appear to “zone out.” Shutdowns carry the same neurological cause as meltdowns but express differently.
| Behavior | Voluntary? | Goal-directed? | Best caregiver response |
|---|---|---|---|
| Meltdown | No | No | Safety, sensory reduction, calm presence |
| Tantrum | Yes | Yes | Consistent boundaries, calm redirection |
| Shutdown | No | No | Quiet presence, reduced demands, patience |
Key signs that distinguish a meltdown from a tantrum:
- Meltdown: no audience awareness, no “checking” for reaction, continues regardless of response
- Meltdown: followed by exhaustion and emotional rawness, not satisfaction
- Tantrum: stops when the goal is achieved or the audience leaves
- Tantrum: child maintains awareness of surroundings throughout
How to manage autism meltdowns step by step
Step-by-step managing of autism meltdowns requires a different response at each phase. The same action that helps during escalation can make a crisis worse.
Before crisis: early escalation response
- Reduce sensory input immediately. Lower lights, move to a quieter space, or remove the stressor if possible.
- Speak in a calm, low, slow voice. Your nervous system directly influences theirs. Caregiver calmness modulates the individual’s nervous state, making your own regulation a clinical tool, not just good manners.
- Offer two concrete choices using a visual coping menu if available. “Do you want headphones or the quiet room?” gives control without cognitive overload.
- Wait 60 seconds between prompts. Silence is not inaction.
During crisis
- Prioritize safety above all else. Remove hazards from the environment rather than restraining the individual.
- Stop all verbal instructions and questions. The brain cannot process them during a full meltdown.
- Avoid physical contact unless the individual invites it or immediate safety requires it. Unexpected touch increases distress.
- Stay present and calm. Your steady presence is the anchor.
After the meltdown: recovery and repair
The post-meltdown period is the best time for learning and prevention planning, but only after the nervous system has fully recovered. Wait until the individual is calm, rested, and regulated before any conversation about what happened. Future for Autism recommends a Regulate, Relate, Reason sequence: calm first, connect second, problem-solve third. Skipping the first two steps makes the third one useless.

Pro Tip: Create a written or visual “calm-down plan” with the individual during a relaxed moment, not after a meltdown. Include their preferred sensory tools, safe spaces, and two or three coping choices. Review it together every few weeks.
For deeper context on supporting communication during recovery, the autism communication strategies guide from Autismdoctorsearch covers practical tools caregivers can use during de-escalation.
How to prevent future meltdowns through environment and routine
Prevention is more effective than any in-the-moment response. Reducing the total sensory and emotional load an individual carries each day lowers the frequency and intensity of meltdowns over time.
Creating an autism-friendly environment at home is one of the highest-impact changes caregivers can make. This means reducing unpredictable noise, using softer lighting, providing a designated quiet space, and minimizing clutter in high-traffic areas. Small physical changes produce measurable reductions in daily stress load.
Practical prevention strategies include:
- Visual schedules: Post a daily schedule with pictures or icons. Predictability reduces anxiety before it builds.
- Transition warnings: Give a five-minute and then a two-minute warning before any activity change. Abrupt transitions are a leading trigger.
- Sensory kits: Prepare a portable kit with noise-canceling headphones, a fidget tool, sunglasses, and a preferred comfort item for outings.
- Collaborative planning with therapists: Occupational therapists and ABA specialists can conduct sensory profiles and build individualized prevention plans. The benefits of occupational therapy for autistic children include exactly this kind of tailored environmental support.
- Ongoing observation: Revisit your trigger log monthly. Triggers shift as children grow and environments change.
Pro Tip: Before any new or unfamiliar event, do a “social story” walkthrough. Describe what will happen, what it will look, sound, and smell like, and what the exit plan is. Preparation reduces the unknown, which is one of the most consistent meltdown triggers.
Caregiver self-regulation is also a prevention tool. Managing your own emotional state before interacting with a dysregulated individual is not optional. Your breathing, voice tone, and body language communicate safety or threat before any words do. Resources on emotional regulation for parents offer practical techniques caregivers can practice independently.
Key Takeaways
Autism meltdowns are involuntary neurological crises requiring sensory reduction, caregiver calm, and phase-specific responses to manage safely and effectively.
| Point | Details |
|---|---|
| Meltdowns are not tantrums | They are involuntary neurological events, so discipline and reasoning make them worse. |
| Phases require different responses | Early escalation allows intervention; crisis phase requires safety focus only. |
| Caregiver calm is a clinical tool | Your regulated nervous system directly reduces the individual’s escalation. |
| Prevention beats reaction | Visual schedules, sensory kits, and routine preparation reduce meltdown frequency. |
| Post-meltdown timing matters | Delay all problem-solving until the nervous system has fully recovered. |
What I’ve learned from watching caregivers get this wrong
The most common mistake I see is caregivers trying to reason with a child who is already in crisis. The impulse makes sense. You want to explain, reassure, and fix it. But the brain in a full meltdown cannot receive that information. You are speaking to a nervous system that has gone offline. Every word you add increases the sensory load.
The second mistake is treating recovery as the end of the episode. The calm after a meltdown is actually the most useful moment in the whole cycle. That is when the nervous system is available again, when connection is possible, and when a child can begin to build self-awareness about their own triggers. Caregivers who skip this window miss the best opportunity for long-term change.
What actually works is less than most people expect. Fewer words. Less movement. More stillness. A calm body next to a dysregulated one is doing real neurological work, even when it looks like nothing. The caregivers who understand this stop feeling helpless during meltdowns because they realize their presence is the intervention.
Meltdowns do not define the individual having them. They are a signal that the nervous system was pushed past its limit. Your job is not to prevent every hard feeling. It is to be a safe, steady presence when the hard feelings arrive. That trust, built over time, is what reduces meltdowns more than any single strategy.
— Keith
Professional autism therapy and support through Autismdoctorsearch
Managing meltdowns at home is more effective when it runs alongside professional support. Applied Behavior Analysis, occupational therapy, and emotional regulation therapy each address different aspects of meltdown prevention and recovery. ABA therapy builds coping skills and communication tools that reduce the frequency of crises over time. Occupational therapists conduct sensory profiles and design environments that lower daily stress load. Autismdoctorsearch maintains a current directory of vetted providers across these specialties. Browse autism therapy services listed on Autismdoctorsearch to find local specialists who can build a plan tailored to your child’s specific triggers and needs.
FAQ
What is an autism meltdown?
An autism meltdown is an involuntary neurological crisis caused by sensory or emotional overload. It is not a deliberate behavior and cannot be stopped through willpower or discipline.
What triggers autism meltdowns most often?
The most common triggers are sensory overload (noise, lights, textures), unexpected routine changes, communication frustration, and accumulated stress from multiple smaller stressors building up over a day.
How should you respond to an autism meltdown in the moment?
Reduce sensory input, stop giving verbal instructions, avoid physical contact unless invited, and stay calm and present. The Child Mind Institute confirms that crisis-phase intervention should focus entirely on safety, not cooperation.
How is a meltdown different from a tantrum?
A meltdown is involuntary and not goal-directed. A tantrum is a purposeful behavior aimed at achieving a specific outcome. Applying consequences during a meltdown increases distress without changing behavior.
When is the right time to talk about a meltdown afterward?
Wait until the nervous system has fully recovered before any discussion. Future for Autism recommends the Regulate, Relate, Reason sequence: calm and connect first, then problem-solve.


