
TL;DR:
- A clinical assessment for autism involves a comprehensive, multi-method process using caregiver interviews, behavioral observations, and standardized testing to confirm a diagnosis based on DSM-5-TR criteria. This evaluation typically lasts several hours across multiple sessions, conducted by a multidisciplinary team that combines diverse expert insights. Early diagnosis enables targeted support and intervention, making thorough assessment essential for effective long-term outcomes.
A clinical assessment for autism is a structured, multi-method evaluation process used to determine whether a child meets the diagnostic criteria for autism spectrum disorder (ASD). Unlike a simple screening, this process combines caregiver interviews, direct behavioral observations, and standardized cognitive and social testing to build a complete picture of your child’s development. No blood test or brain scan can diagnose autism. The process relies entirely on clinical judgment applied to DSM-5-TR criteria, which center on persistent social communication deficits and restricted, repetitive behaviors. Understanding what this process involves helps you prepare, advocate, and move forward with confidence.
What is clinical assessment for autism?
Clinical assessment for autism is the formal diagnostic process that moves beyond initial screening to confirm or rule out ASD through a thorough, evidence-based evaluation. The American Psychiatric Association’s DSM-5-TR defines the two core symptom domains that clinicians assess: deficits in social communication and interaction, and the presence of restricted or repetitive patterns of behavior. Both must be present across multiple contexts and must have appeared in early development, even if they were not fully recognized at the time.
The process is not a single appointment. A comprehensive autism evaluation typically lasts 2 to 4 hours and often spans multiple sessions. Clinicians gather data from three primary sources: what caregivers report, what they directly observe in the child, and what standardized tests reveal. Each source fills gaps the others cannot. A child who masks well in a clinical setting may show clear patterns at home, and vice versa. That is why no single data point drives the diagnosis.
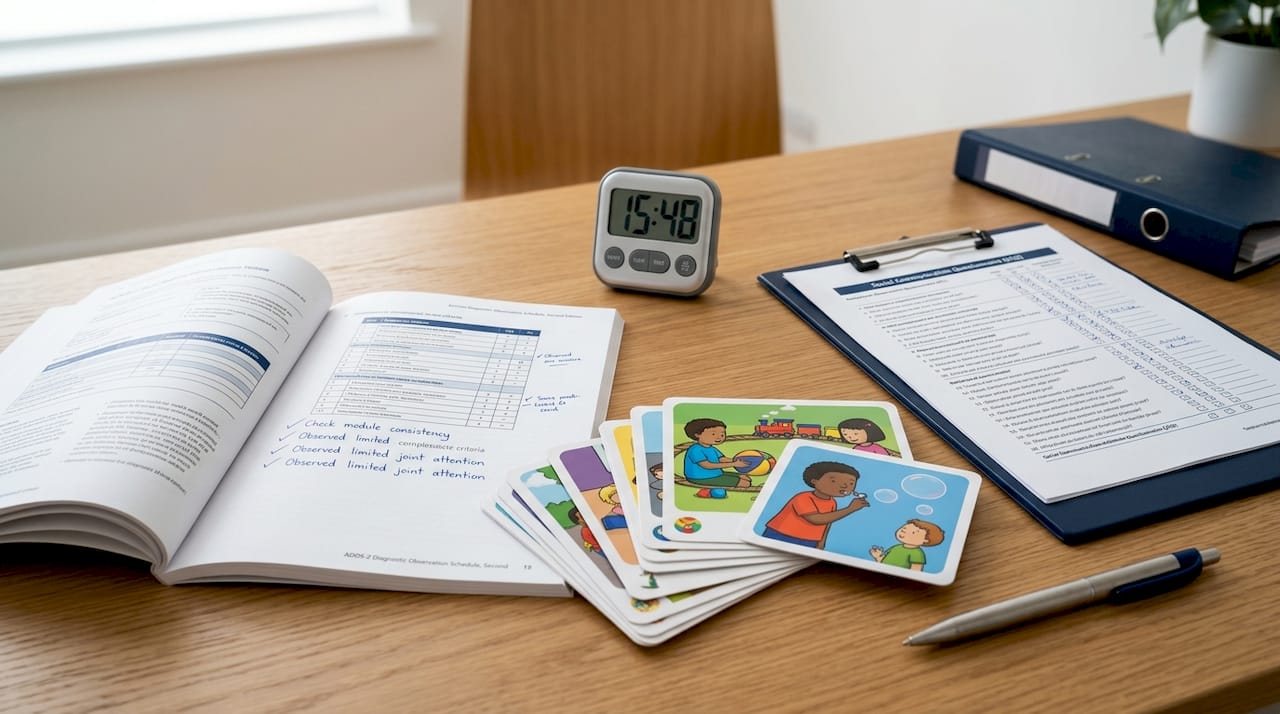
The gold-standard tools used in most clinical settings are the ADOS-2 (Autism Diagnostic Observation Schedule, Second Edition) and the ADI-R (Autism Diagnostic Interview, Revised). The ADOS-2 and ADI-R are structured instruments that give clinicians a consistent, research-validated framework for observing social behavior and gathering developmental history. Their combined use significantly reduces the risk of misdiagnosis.
What happens during the autism evaluation process?
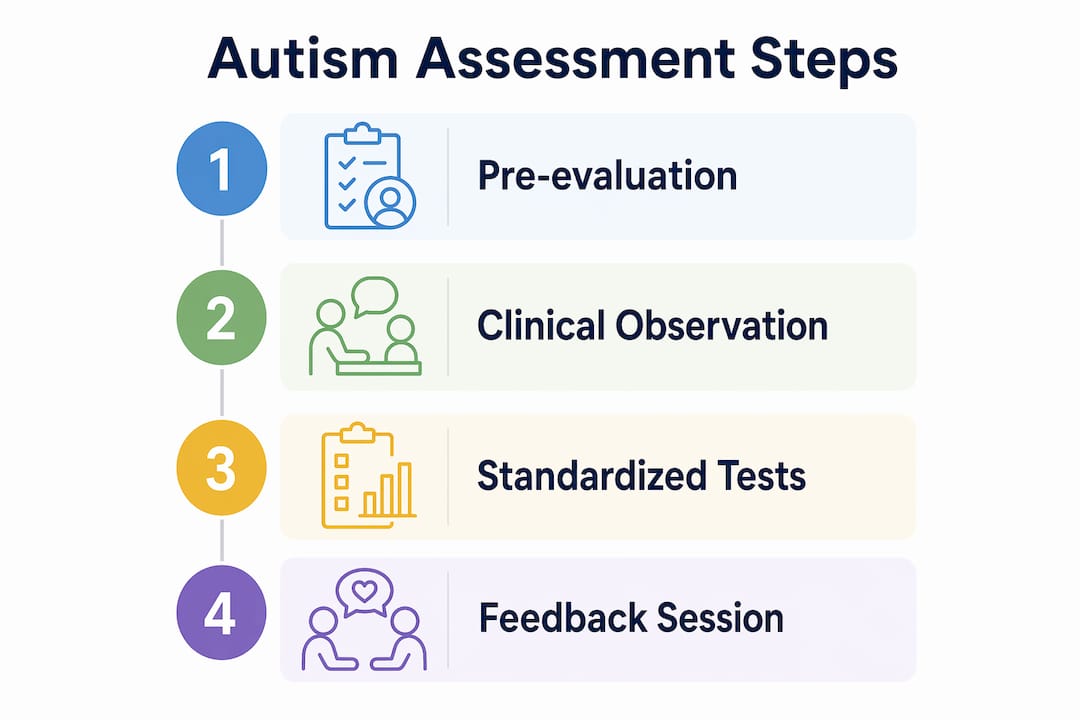
The autism evaluation process follows a structured sequence, though the exact order varies by clinic and provider team. Here is what most families can expect:
- Referral and intake. Your child’s pediatrician or a school professional typically initiates the referral. You will complete intake forms covering developmental milestones, medical history, and current concerns.
- Caregiver interview (ADI-R). A clinician conducts a detailed interview with parents or caregivers, often lasting 90 minutes or more. This covers early development, language acquisition, social behavior, and daily routines.
- Direct observation (ADOS-2). The clinician engages your child in structured play and conversation activities designed to elicit social communication behaviors. This session is scored against standardized benchmarks.
- Developmental and cognitive testing. Psychologists administer tests measuring IQ, language ability, adaptive behavior, and executive function. These results clarify your child’s strengths and support needs.
- Specialist consultations. Depending on the clinic, speech-language pathologists assess communication, and occupational therapists evaluate sensory processing and motor skills.
- Feedback session. The team reviews all findings with you, explains the diagnosis or outcome, and outlines recommended next steps.
Specialists involved typically include developmental pediatricians, clinical psychologists, speech-language pathologists, and occupational therapists. Each professional contributes a distinct lens. A multidisciplinary team approach is preferred because it rules out conditions with overlapping symptoms, such as ADHD, anxiety disorders, or language delays, that a single clinician might miss.
Pro Tip: Before your child’s first session, write down three to five specific behavioral examples from different settings, such as home, school, and social gatherings. Clinicians use these concrete observations to differentiate autism from other developmental conditions.
How does autism screening differ from clinical assessment?
Screening and clinical assessment serve different purposes, and confusing the two is one of the most common sources of parental anxiety. Here is how they compare:
| Feature | Autism screening | Clinical assessment |
|---|---|---|
| Purpose | Identifies children at risk | Confirms or rules out ASD diagnosis |
| Duration | 5 to 20 minutes | 2 to 4 hours across multiple sessions |
| Tools used | M-CHAT-R/F, ASQ-3, brief checklists | ADOS-2, ADI-R, cognitive and adaptive tests |
| Who conducts it | Pediatrician or primary care provider | Multidisciplinary specialist team |
| Outcome | Risk indicator, not a diagnosis | Clinical diagnosis with written report |
The CDC recommends autism screening at 18 and 24 months during routine well-child visits, with developmental surveillance at every visit from birth onward. A reliable diagnosis can be made as early as age 2, which matters because earlier intervention produces better long-term outcomes.
A positive screening result does not mean your child has autism. Positive screening results indicate that a full evaluation is warranted, not that a diagnosis is certain. Many children who screen positive do not receive an ASD diagnosis after comprehensive assessment. The screening simply flags a pattern worth investigating.
Key reasons both steps matter:
- Screening catches children who might otherwise go unnoticed until school age.
- Clinical assessment provides the detailed profile needed to design effective interventions.
- Early diagnosis following assessment opens access to speech therapy, ABA therapy, occupational therapy, and special education services.
- Without a formal diagnosis from clinical assessment, many insurance plans and school districts will not fund support services.
You can learn more about the early screening process and what to expect at each developmental stage in Autismdoctorsearch’s parent guide.
Common challenges families face and how to prepare
The autism evaluation process is thorough, and that thoroughness comes with real logistical and emotional demands. Knowing what to expect reduces stress for both you and your child.
Scheduling and wait times. Specialist waitlists for autism evaluations can stretch from several months to over a year in many regions. Request referrals as soon as concerns arise. While waiting for a private or hospital-based evaluation, request a school-based evaluation simultaneously. Under the Individuals with Disabilities Education Act (IDEA), public schools are legally required to evaluate children suspected of having a disability at no cost to the family. School-based evaluations under IDEA do not replace a clinical diagnosis but provide timely access to educational supports while you wait.
Insurance barriers. Insurance companies sometimes deny initial requests for autism testing. This is not the end of the road. You can appeal through a medical necessity letter from your child’s pediatrician, and you have the right to escalate unresolved denials to your state insurance commissioner. Autismdoctorsearch has a detailed resource on navigating insurance appeals that walks you through each step.
Keeping your child comfortable during sessions. Diagnostic sessions are taxing for children, particularly those with sensory sensitivities or anxiety. Schedule appointments during your child’s most alert and regulated time of day. Bring a preferred comfort item, a familiar snack, and noise-canceling headphones if your child uses them. Let the clinician know about any sensory triggers before the session begins.
Completing pre-evaluation questionnaires accurately. These forms are not administrative paperwork. Pre-evaluation questionnaires are critical diagnostic data points that clinicians weigh alongside direct observation. Note specific behaviors from multiple environments, including home, school, and community settings. Vague answers like “sometimes has tantrums” are far less useful than “has a 20-minute meltdown when transitions happen without a five-minute warning, three to four times per week.”
Pro Tip: Ask your child’s teacher to complete a behavioral questionnaire as well. Teacher observations from a structured school environment often reveal patterns that parents do not see at home, and clinicians value data from multiple informants.
How multidisciplinary teams improve assessment accuracy
A single clinician, no matter how skilled, cannot fully capture the complexity of autism. The diagnostic accuracy improves substantially when a coordinated team pools findings from different professional perspectives.
Here is what each specialist contributes:
- Developmental pediatrician or child psychiatrist: Reviews medical history, rules out genetic or neurological conditions, and oversees the overall diagnostic process.
- Clinical psychologist: Administers the ADOS-2, ADI-R, and cognitive assessments. Interprets behavioral patterns against DSM-5 criteria.
- Speech-language pathologist: Evaluates receptive and expressive language, pragmatic communication, and social use of language.
- Occupational therapist: Assesses sensory processing, fine motor skills, and daily living abilities. Occupational therapists who practice from a neurodiversity-affirming framework focus on supporting the child’s strengths rather than eliminating differences.
The team shares findings before the feedback session, which means the diagnosis you receive reflects integrated data rather than one professional’s impression. This process also catches co-occurring conditions. Roughly 70% of autistic individuals have at least one co-occurring condition, such as ADHD, anxiety, or intellectual disability. A multidisciplinary team is far better positioned to identify these overlapping presentations than a solo evaluator.
After diagnosis, the same team structure informs intervention planning. The psychologist’s cognitive profile guides academic accommodations. The speech therapist’s findings shape communication goals. The occupational therapist’s report informs sensory supports. You can explore how coordinated autism care benefits families beyond the assessment itself through Autismdoctorsearch’s dedicated resource.
Key takeaways
A clinical assessment for autism requires multiple data sources, specialist expertise, and structured tools to produce a diagnosis that is both accurate and actionable.
| Point | Details |
|---|---|
| No single test diagnoses autism | Diagnosis depends on integrated clinical judgment using DSM-5-TR criteria, not lab results. |
| Gold-standard tools are ADOS-2 and ADI-R | These structured instruments reduce misdiagnosis when combined with developmental history. |
| Screening is not diagnosis | A positive M-CHAT-R/F or ASQ-3 result triggers referral for full clinical assessment. |
| Multidisciplinary teams improve accuracy | Developmental pediatricians, psychologists, speech therapists, and OTs each contribute distinct findings. |
| Preparation directly affects outcomes | Detailed behavioral examples and accurate questionnaires help clinicians make more precise diagnoses. |
What I’ve learned from watching families navigate this process
The families who come through the autism assessment process most successfully share one trait: they treat the evaluation as a collaboration, not a verdict. I have seen parents arrive at feedback sessions braced for the worst, only to leave with a clear map of their child’s strengths and a concrete intervention plan. The diagnosis is not the end of something. It is the beginning of targeted support.
One thing I wish more parents knew before the process starts: the waiting period between referral and evaluation is not wasted time. Use it to document your child’s behavior across settings, gather school reports, and connect with other families who have been through the process. The more specific and detailed the information you bring into the evaluation, the more useful the outcome will be.
I also want to address the fear that a diagnosis will limit your child. The opposite is true. Without a clinical assessment, children often spend years receiving generic support that does not match their actual profile. A thorough evaluation gives clinicians, teachers, and therapists the specific information they need to help your child in ways that actually work. Advocating for a complete assessment is one of the most concrete things you can do for your child right now.
— Keith
Find trusted autism evaluation and therapy providers
Autismdoctorsearch connects families with specialized autism evaluation centers, therapy providers, and multidisciplinary clinics across the country. Whether you are at the beginning of the assessment process or looking for post-diagnosis support services, the directory makes it straightforward to find providers who specialize in ABA therapy, occupational therapy, speech therapy, and more. Browse the autism therapy services directory to find trusted professionals near you and take the next step toward getting your child the support they need.
FAQ
What is the difference between autism screening and clinical assessment?
Screening is a brief risk-detection tool administered by a pediatrician, while clinical assessment is a comprehensive diagnostic evaluation conducted by a specialist team. A positive screening result means your child needs a full evaluation, not that they have autism.
How long does a clinical autism assessment take?
A clinical autism evaluation typically lasts 2 to 4 hours and often spans more than one appointment. The total time depends on the number of specialists involved and the complexity of your child’s presentation.
What tools do clinicians use to diagnose autism?
The ADOS-2 and ADI-R are the gold-standard diagnostic instruments used in most clinical settings. These are combined with cognitive tests, adaptive behavior scales, and developmental history reviews to produce a complete diagnostic picture.
Can a school evaluation replace a clinical autism assessment?
A school-based evaluation under IDEA determines eligibility for educational services but does not constitute a medical diagnosis. A clinical assessment from a qualified specialist team is required for an official ASD diagnosis and insurance-funded services.
What should I bring to my child’s autism evaluation?
Bring completed questionnaires with specific behavioral examples from multiple settings, any previous developmental or school reports, a comfort item for your child, and a list of questions for the feedback session. The more concrete your behavioral documentation, the more useful it is to the clinical team.


